Spondylolisthesis results in neurological symptoms due to instability and canal and lateral recess stenosis.
Surgical treatment consists of decompression and fusion. Various fusion methods have been described such as intertransverse fusion, PLIF and TLIF.
Key-hole methods can be used to TLIF. Bilateral decompression and fusion alongwith fixation is achieved using Minimally invasive methods. Tubular access channels are used for exposing the level of interest. This tube can be manipulated in supero-inferior and medio-lateral direction to achieve upto 2 level decompression and unilateral as well as bilateral decompression through the same one sided incision.
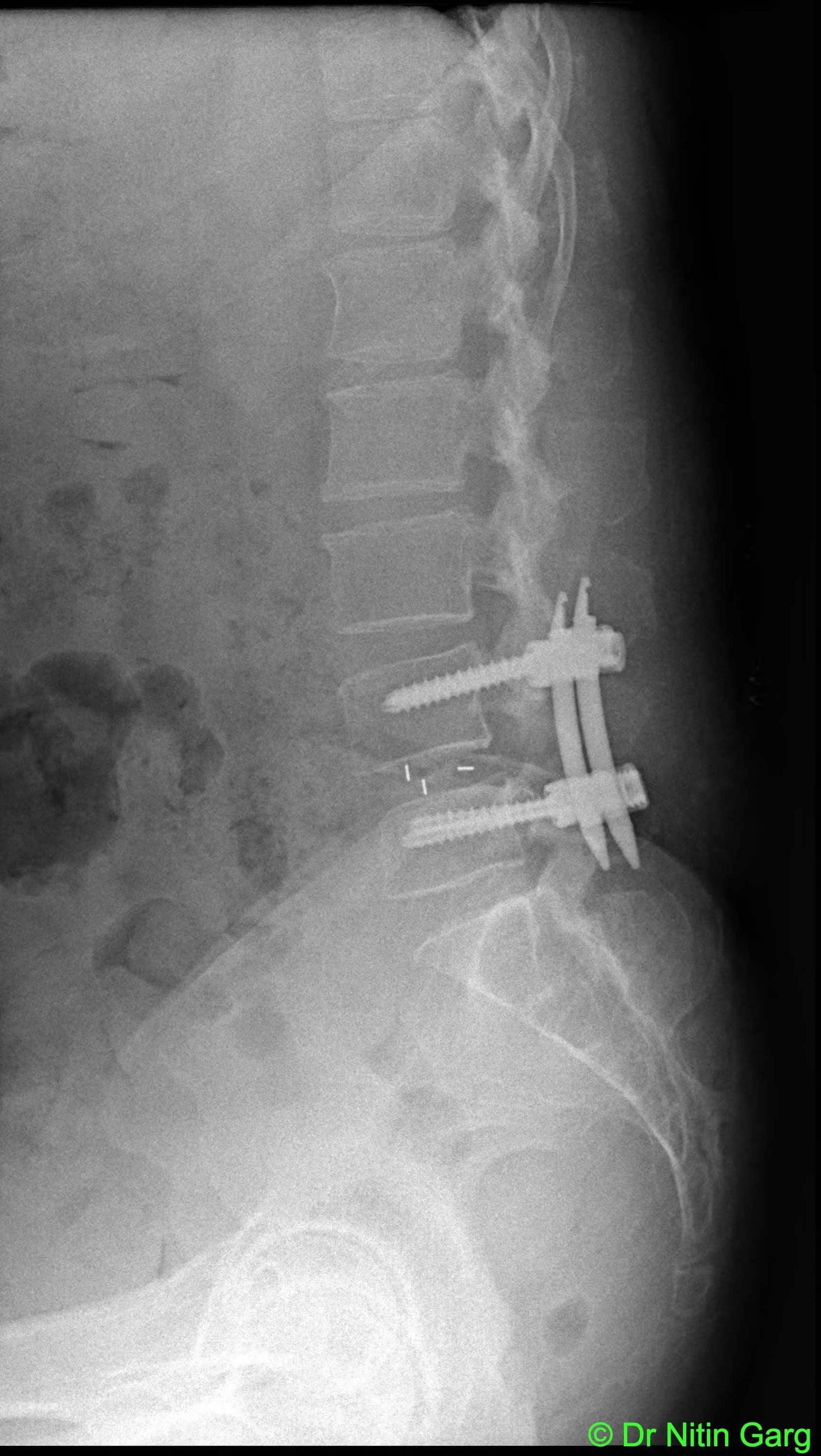
This patient had L4-5 degenerative spondylolisthesis with significant ligamentum flavum and facetal hypertrophy causing bilateral lateral recess stenosis. He underwent Minimally invasive TLIF using tubular ports. Post-op recovery was uneventful.

Pre-op X-ray -- L4-5 spondylolisthesis

Sagittal T2W MRI with L4-5 canal stenosis

Axial T2W image with bilateral lateral recess stenosis
.jpg)
Follow up MRI shows adequate canal decompression
_1.jpg)
Follow up MRI -- bilateral canal decompressed by unilateral approach. Muscle bulk/ bony anatomy maintained.